
Antihistamines as a sleep aid with adjunctives and synergizers.
Blog homepage: http://lysanderdusseljee.blogspot.com/
This paper as as commentable google doc.
This paper as a published google doc.
Lysander Dusseljee
Professor Name removed for public viewing
Chem 131
December 2, 2016
Prelude
Insomnia, in addition to being a nuisance, puts one at serious risk and disadvantage. According to the Centers for Disease Control and Prevention (CDC), nearly 10% of the U.S. population experiences chronic insomnia (1). The CDC further states that insufficient sleep is associated with metabolic diseases such as diabetes and obesity (1). However, it is the association between insomnia, as well as other sleep disturbances, and depression that particularly interests me. In patients with major depression, hypersomnia and insomnia are associated with suicidal behavior (2). It is, however, debatable in my opinion whether or not hypersomnia is just another form of sleep insufficiency. For example, sodium oxybate is a sleep aid that enhances objective measures of sleep architecture and is indicated by the FDA for the treatment of excessive daytime sleepiness in patients with narcolepsy (3). Nevertheless, since hypersomnia is associated with increased slow wave sleep (SWS), the objective quality of sleep in hypersomniacs can be debated, (4).
What’s more, sleep is important for cognitive performance in several domains. A recent study found that autonomic nervous system (ANS) activity during sleep, in conjunction with electroencephalogram (EEG) sleep parameters, was able to predict over half of the variance for memory consolidation after a nap (5). Since drugs can be used to modify both EEG parameters and ANS activity, it should be possible to use drugs to both treat sleep conditions and enhance sleep beyond baseline in normal sleepers. Thus, I have set out to achieve both of these goals for myself. That is to say, I wish to become a normal sleeper, then continue to improve sleep to the maximum extent possible.
Abstract
In recent years, I have experimented with several over the counter (OTC) and unregulated drugs. In particular, I have focused on attempting to treat my extended sleep onset latency and daytime sleepiness. While this wouldn’t be technically difficult if I had unlimited access to prescription drugs, the use of OTC substances allows for greater access and utilization. I find physicians, even specialists, to be neither knowledgeable nor competent. Thus, my most recent attempts have involved the OTC antihistamine doxylamine in combination with the acetylcholinesterase inhibitor huperzine-A. I have, however, also recently started taking the research chemical ibutamoren, often referred to as MK-677, which is an unregulated ghrelin receptor agonist and growth hormone secretagogue that appears to improve sleep architecture (6). This could potentially confound the results. I may, in the future, attempt a blinded, placebo controlled, crossover self experiment to reduce confounding factors.
Methods
Doxylamine, huperzine A, melatonin, and methylxanthines were administered in an ad libitum yet experimental fashion for a period of about 4 weeks. MK-677 was also taken during this time, but this was incidental and unrelated to this specific experiment. Likewise, while melatonin is an intentional adjunct, it is not intended to work via the same mechanisms. Doxylamine doses ranged from 25 mg to 150 mg, with a median dose of 50mg. Huperzine A doses ranged from 200 mcg to 800 mcg, with a median dose of 200 mcg. Melatonin was generally administered as a 6 hour slow release 300 mcg tablet, with the exception of a short period where my supply ran out and I had to settle for 300 mcg rapid release melatonin. Morning caffeine and/or theobromine was administered at various doses during the most recent week of this experiment. Doxylamine, huperzine A, and melatonin were all administered at the same time, generally several hours before desired bedtime. The past few days, however, I have opted to administer huperzine A in the mornings. Caffeine doses ranged from 200 mg to 400 mg, and theobromine doses ranged from 550 mg to 1300 mg. The combined dose of 200 mg caffeine and 550 mg theobromine was not exceeded during any given day. The experiment continues up to and after the release of this paper.
Update: my current regimen, as of December 19, 2016, is stable at high end for doxylamine at 150 mg. I’m also taking 50 mg of meclizine as well, but this is mostly incidental, since it happens to be in the capsules I made (for its shorter half life). This has been mostly sufficient for sleep, but I still often maintain moderate sleep onset latency. It causes an intense warm and occasional tingly sensation that I assume is due to the anticholinergic effects such as reduced sweating. While there is sometimes the sensation of sensation of sweating, sweat appears absent to the touch. A man hospitalized for a doxylamine overdose suicide attempt (1 bottle = 96 * 25 mg tabs = 2400 mg) was reported as “warm to touch”. While 150 mg should be well below the danger level, particularly considering that I’m taking huperzine A, it’s still approaching levels of anticholinergic activity which would be best to avoided. Not the least of which because, though causality is not necessarily implicated, long term anticholinergic use is associated with increased risk of dementia (causal, exacerbatory, or correlation are all possible. They controlled for sleep disorders by looking at benzodiazepine use, so I consider sleep disorders to be poorly controlled for).
Update 2: I am no longer taking this stack. It was not effective enough to be worth the side effects. I have since achieved roughly equivalent (if poor) sleep by other means. I’m currently pursuing a hydroxyzine prescription, which appears mechanistically promising, safe, and relatively side effect free. 200-300 mg is the dose range I’m interested in, as that dose should remain effective at peak tolerance. I am still interested in and experimenting with aspects of this stack (e.g. methylxanthines and melatonin), but much of it I suspect would be more effective after I solve my cardiovascular abnormalities (i.e. tachycardia) via blood/plasma volume expansion.
Discussion
Histaminergic neurons in the central nervous system (CNS), located exclusively in the posterior hypothalamus, play a major role in sleep-wake regulation, (7). The wake promoting effects of histamine are mediated through H1 and H2 receptors, while the H3 receptor functions as an autoreceptor providing a negative feedback loop, (7). Thus, H1 and H2 receptor antagonists, and H3 receptor agonists, promote sleep, (7). Further, impairment of histaminergic neurotransmission improves sleep architecture by increasing SWS, (7). Centrally active H1 and H2 receptor antagonist are able to increase SWS, (7,8). Doxylamine is a first-generation antihistamine, active as an antagonist at the H1 receptor, that is commonly used as a potent OTC sleep aid at 25mg, (9,10). I have chosen doxylamine over diphenhydramine for its potency and comparatively short half-life of around a dozen hours, (9,10). [One reason I've avoided diphenhydramine is not the half life per se., but the half life variation between individuals. I want the greatest consistent applicability.]
Doxylamine, like other antihistamines, possesses anticholinergic properties, (11). While low acetylcholine is associated with SWS, high acetylcholine is associated with rapid eye movement (REM) sleep and wakefulness, (12). Further, low cholinergic tone appears important for memory consolidation during SWS, (12). In contrast, reduced acetylcholine during wakefulness is associated with cognitive deficits, (13). Further, REM sleep is associated with even higher acetylcholine levels than wakefulness, (13). Huperzine A is a naturally occurring, potent, OTC cholinesterase inhibitor that increases acetylcholine levels and appears to enhance cognition in cognitively impaired and healthy subjects alike, (14,15). Thus, huperzine A can be used to counteract the anticholinergic side effects of doxylamine. However, the combined effects of doxylamine and huperzine A on cholinergic neurotransmission is unclear. Nevertheless, I speculate that the combination should be net positive with regards to modulating cholinergic neurotransmission in a sleep stage targeted manner.
Acetylcholine plays a significant role in the ANS, (16). There are two main classes of acetylcholine receptors in both the central and peripheral nervous systems, (16). Namely, the two main classes of acetylcholine receptors are the nicotinic-acetylcholine receptors and the muscarinic-acetylcholine receptors, (16). First generation antihistamines, like doxylamine, are muscarinic-acetylcholine receptor antagonists, (17). These antimuscarinic effects can cause dry mouth, tachycardia, thickening of mucus, and may play a role in the sedating properties of antihistamines, (18).
Nicotine is a nicotinic-acetylcholine receptor agonist that interacts with the ANS via several nicotinic receptor subtypes, (19). The ANS is divided into two divisions; the sympathetic and parasympathetic divisions, (20). The sympathetic nervous system (SNS) is commonly characterized by the “fight-or-flight” response, (20). The parasympathetic nervous system (PSNS) is commonly characterized by “rest and digest” functions, (20). Nicotine possesses both sympathomimetic and parasympathomimetic properties, (19). Nicotine increases REM sleep in low doses and decreases REM sleep in high doses in both rats and humans, (21-26). Additionally, long term administration of low dose nicotine is able to increase SWS in depressed patients, (27). These sleep enhancing and sleep impairing effects of nicotine are likely due to PSNS activation and SNS activation respectively.
Caffeine causes histamine release in the brain through downstream mechanisms of adenosine receptor antagonism, (28). Thus, increased histaminergic tone appears to be one of the mechanisms by which caffeine promotes wakefulness. Tolerance to the sedating effects of antihistamines develops extremely rapidly, with complete tolerance to the sedating effects of diphenhydramine occurring by the end of 3 days of twice daily administration, (29). Likewise, caffeine tolerance appears to develop rapidly, with near complete tolerance to the cortisol elevating effects occurring within 5 days of twice daily administration, (30). Further, an adenosine A2A receptor agonist, the opposite of caffeine, causes downstream histaminergic inhibition, (31). Further still, chronic caffeine administration is able to increase SWS in rats, (32). This is presumably due to caffeine tolerance and subsequent caffeine withdrawal during the sleep phase. Thus, antihistamines and caffeine may be able to help prevent tolerance to one another. Consequently, taking caffeine in the morning and doxylamine at night should improve sleep architecture via several mechanisms. Thus, I have added morning caffeine to my experiment. However, the half-life of caffeine varies dramatically between individuals, so may influence people differently, (33,34).
Theobromine, like caffeine, is an adenosine receptor antagonist, but with two and three fold lower affinity for the A1 and A2A receptors respectively, (35). However, theobromine is only about 15% lower potency than caffeine as a phosphodiesterase inhibitor, (36). The wide ranging implications of phosphodiesterase inhibitors are beyond the scope of this paper. However, for our purposes, the primary implication of this disparity involves the effects on vasoaction, heart rate, and ANS activity. Due to the vasoconstriction caused by adenosine receptor antagonism, caffeine causes an increase in blood pressure, reduced heart rate, and reduced blood flow, (37-39). In contrast, theobromine causes vasodilation via phosphodiesterase inhibition, resulting in reduced blood pressure, increased heart rate, and minimal impact on blood flow, (35,40). The primary implications of this are that caffeine, but not theobromine, may inhibit blood volume expansion, such as that induced by exercise, (41). Whether the vasodilation caused by theobromine is sufficient to induce blood volume expansion is unclear, but chronic vasodilation in general causes volume expansion of the plasma portion of the blood, (42,43). Conversely, chronic vasoconstriction is sufficient to reduce blood volume, (44-46). Thus, I have added theobromine to my experiment as an alternative to, and complement of, caffeine.
Figure 1
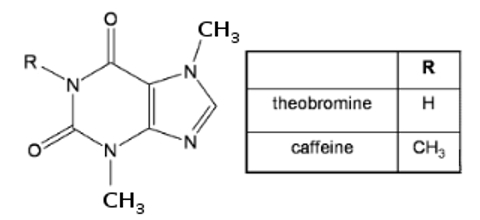
Figure 1: Caffeine and theobromine molecular structures. Adapted
from Callahan et al., (47).
from Callahan et al., (47).
However, while caffeine is water soluble and peaks 30-40 minutes post-ingestion, theobromine is lipid soluble and peaks in 2-3 hours, (35). This is surprising given that the only difference between caffeine and theobromine is that, where caffeine has a methyl substituted 3° amide, theobromine has a 2° amide available for hydrogen bonding (see Figure 1 above), (47). This appears to result in the dimerization and subsequent lipophilicity of theobromine, (47). Since the lipophilicity of theobromine results in a longer absorption duration, I have not completely substituted theobromine for caffeine. Rather, I am combining 200 mg caffeine with 550 mg theobromine in one dose, resulting in rapid yet relatively stable adenosine receptor antagonism for several hours. In the near future, I intend to add a fast acting vasodilator to counteract the vasoconstriction caused by caffeine.
Given that huperzine A increases acetylcholine, and thus both nicotinic and muscarinic tone, and given that doxylamine decreases muscarinic tone specifically, I would expect the combination of the two to primarily increase nicotinic tone specifically overall. Provided that the huperzine A dose used isn’t too high, I also expect that this combination will provide the same benefits as low dose nicotine for sleep. Additionally, I would expect that the brain is still capable of lowering acetylcholine levels to some extent during SWS, even in the presence of huperzine A, yet huperzine A will certainly enhance acetylcholine elevations during REM. If this is the case, then I would expect the combination of doxylamine and huperzine A to decrease muscarinic tone during SWS, and increase nicotinic tone during REM sleep.
Results
This combination generally seems to reduce sleep onset latency and increase sleepiness. However, when the doxylamine dose is insufficient relative to my tolerance, I can end up staying awake well after plasma concentration peaks. Caffeine and theobromine appear to have been somewhat effective at reducing my tolerance to doxylamine’s sleep promoting effects.
Huperzine A seems to reduce doxylamine side effects, such as dry mouth. However, since huperzine A peaks faster than doxylamine, it seems to induce cholinergic side effects such as sweating. However, I tend to sweat at night, especially after melatonin, so this effect may simply be an exacerbation my symptoms and may not be a side effect for everyone. The details of why melatonin might cause sweating is beyond the scope of this paper, but presumably involves the implications vasodilation on SNS activation.
While, in the context of combination with doxylamine specifically, 200 mcg of huperzine A may slightly enhance dream recall, 400 mcg displays a pronounced increase in dream recall. However, I no longer remember these dreams, but there was a reasonable period post-waking to write them down, if so desired.
Conclusions
While I cannot say for certain that this is an objectively good combination, it is objectively beneficial to the best of my knowledge. The subjective results so far appear promising. Huperzine A is capable of reducing the anticholinergic side effects of doxylamine. The adenosine receptor antagonists caffeine and theobromine appear capable of reducing tolerance to the sedating effect of antihistamines, though whether this is due to direct or indirect mechanisms should be further elucidated.
References
(1) Sleep and Sleep Disorders http://www.cdc.gov/sleep/index.html (accessed Nov 13, 2016).
(2) YoEargon, M.; Kara, H.; Solmaz, M. Sleep Disturbances And Suicidal Behavior In Patients With Major Depression. The Journal of Clinical Psychiatry 1997, 58, 249-251.
(3) Alshaikh, M.; Tricco, A.; Tashkandi, M.; Mamdani, M.; Straus, S.; BaHammam, A. Sodium Oxybate For Narcolepsy With Cataplexy: Systematic Review And Meta-Analysis. Journal of Clinical Sleep Medicine 2012.
(4) Anderson, K. N.; Pilsworth, S.; Sharples, L. D.; Smith, I. E.; Shneerson, J. M. Idiopathic Hypersomnia: A Study of 77 Cases. Sleep, 2007, 30(10), 1274–1281.
(5) Whitehurst, L.; Cellini, N.; McDevitt, E.; Duggan, K.; Mednick, S. Autonomic Activity During Sleep Predicts Memory Consolidation In Humans. Proceedings of the National Academy of Sciences2016, 113, 7272-7277.
(6) Copinschi, G.; Leproult, R.; Van Onderbergen, A.; Caufriez, A.; Cole, K.; Schilling, L.; Mendel, C.; De Lepeleire, I.; Bolognese, J.; Van Cauter, E. Prolonged Oral Treatment With MK-677, A Novel Growth Hormone Secretagogue, Improves Sleep Quality In Man. Neuroendocrinology 1997, 66, 278-286.
(7) Lin, J.; Sergeeva, O.; Haas, H. Histamine H3 Receptors And Sleep-Wake Regulation. Journal of Pharmacology and Experimental Therapeutics 2010, 336, 17-23
(8) Ikeda-Sagara, M.; Ozaki, T.; Shahid, M.; Morioka, E.; Wada, K.; Honda, K.; Hori, A.; Matsuya, Y.; Toyooka, N.; Ikeda, M. Induction Of Prolonged, Continuous Slow-Wave Sleep By Blocking Cerebral H1 Histamine Receptors In Rats. British Journal of Pharmacology 2011, 165, 167-182.
(9) Videla, S.; Lahjou, M.; Guibord, P.; Xu, Z.; Tolrà, C.; Encina, G.; Sicard, E.; Sans, A. Food Effects On The Pharmacokinetics Of Doxylamine Hydrogen Succinate 25 Mg Film-Coated Tablets. Drugs R D2012, 12, 217-225.
(10) Videla, S.; Cebrecos, J.; Lahjou, M.; Wagner, F.; Guibord, P.; Xu, Z.; Cabot, A.; Encabo, M.; Encina, G.; Sicard, E. et al. Pharmacokinetic Dose Proportionality Between Two Strengths (12.5 Mg And 25 Mg) Of Doxylamine Hydrogen Succinate Film-Coated Tablets In Fasting State: A Single-Dose, Randomized, Two-Period Crossover Study In Healthy Volunteers. Drugs in R&D 2013, 13, 129-135.
(11) Syed, H.; Som, S.; Khan, N.; Faltas, W. Doxylamine Toxicity: Seizure, Rhabdomyolysis And False Positive Urine Drug Screen For Methadone. Case Reports 2009, 280(2), 598-601.
(12) Gais, S.Born, J. Low Acetylcholine During Slow-Wave Sleep Is Critical For Declarative Memory Consolidation. Proceedings of the National Academy of Sciences 2004, 101, 2140-2144.
(13) Vazquez, J; Baghdoyan, H. Basal forebrain acetylcholine release during REM sleep is significantly greater than during waking. American Journal Of Physiology - Regulatory, Integrative And Comparative Physiology 2001, 280(2), R598-R601.
(14) Yang, G.; Wang, Y.; Tian, J.; Liu, J. Huperzine A For Alzheimer’S Disease: A Systematic Review And Meta-Analysis Of Randomized Clinical Trials. PLoS ONE 2013, 8, e74916.
(15) Sun, Q. Q., Xu, S. S.; Pan, J. L.; Guo, H. M.; Cao, W. Q. Huperzine-A capsules enhance memory and learning performance in 34 pairs of matched adolescent students. Zhongguo yao li xue bao= Acta pharmacologica Sinica 1999, 20(7), 601-603.
(16) Tiwari, P.; Dwivedi, S.; Singh, M.; Mishra, R.; Chandy, A. Basic And Modern Concepts On Cholinergic Receptor: A Review. Asian Pacific Journal of Tropical Disease 2013, 3, 413-420.
(17) Church, M.Church, D. Pharmacology Of Antihistamines. Indian Journal of Dermatology 2013, 58, 219.
(18) Liu, H.; Zheng, Q.; Farley, J. Antimuscarinic Actions Of Antihistamines On The Heart. Journal of Biomedical Science 2006, 13, 395-401.
(19) Li, Y.; LaCroix, C.; Freeling, J. Specific Subtypes Of Nicotinic Cholinergic Receptors Involved In Sympathetic And Parasympathetic Cardiovascular Responses. Neuroscience Letters 2009, 462, 20-23.
(20) McCorry, L. K. Physiology of the Autonomic Nervous System. American Journal of Pharmaceutical Education 2007, 71(4), 78.
(21) Salin-Pascual, R.; Moro-Lopez, M.; Gonzalez-Sanchez, H.; Blanco-Centurion, C. Changes In Sleep After Acute And Repeated Administration Of Nicotine In The Rat. Psychopharmacology 1999, 145, 133-138.
(22) Cabeza, R. Are nicotinic receptors involved in regulating REM sleep architecture of the rat?.
(23) Salin-Pascual, R. J. Relationship between mood improvement and sleep changes with acute nicotine administration in non-smoking major depressed patients. Revista de investigacion clinica; organo del Hospital de Enfermedades de la Nutricion 2001, 54(1), 36-40.
(24) Salín-Pascual, R.Drucker-Colín, R. A Novel Effect Of Nicotine On Mood And Sleep In Major Depression. NeuroReport 1998, 9, 57-60.
(25) Jaehne, A.; Unbehaun, T.; Feige, B.; Riemann, D. The Influence Of 8 And 16 Mg Nicotine Patches On Sleep In Healthy Non-Smokers. Pharmacopsychiatry 2014, 47, 73-78.
(26) Gillin, J.; Lardon, M.; Ruiz, C.; Golshan, S.; Salin-Pascual, R. Dose-Dependent Effects Of Transdermal Nicotine On Early Morning Awakening And Rapid Eye Movement Sleep Time In Nonsmoking Normal Volunteers. Journal of Clinical Psychopharmacology 1994, 14, 264-267.
(27) Haro, R.Drucker-Colín, R. Effects Of Long-Term Administration Of Nicotine And Fluoxetine On Sleep In Depressed Patients. Archives of Medical Research 2004, 35, 499-506.
(28) John, J.; Kodama, T.; Siegel, J. Caffeine Promotes Glutamate And Histamine Release In The Posterior Hypothalamus. American Journal of Physiology - Regulatory, Integrative and Comparative Physiology 2014, 307, R704-R710.
(29) Richardson, G.; Roehrs, T.; Rosenthal, L.; Koshorek, G.; Roth, T. Tolerance To Daytime Sedative Effects Of H1 Antihistamines. Journal of Clinical Psychopharmacology 2002, 22, 511-515.
(30) Lovallo, W.; Whitsett, T.; al’Absi, M.; Sung, B.; Vincent, A.; Wilson, M. Caffeine Stimulation Of Cortisol Secretion Across The Waking Hours In Relation To Caffeine Intake Levels. Psychosomatic Medicine 2005, 67, 734-739.
(31) Hong, Z.; Huang, Z.; Qu, W.; Eguchi, N.; Urade, Y.; Hayaishi, O. An Adenosine A2A Receptor Agonist Induces Sleep By Increasing GABA Release In The Tuberomammillary Nucleus To Inhibit Histaminergic Systems In Rats. Journal of Neurochemistry 2005, 92, 1542-1549.
(32) Olini, N.; Kurth, S.; Huber, R. The Effects Of Caffeine On Sleep And Maturational Markers In The Rat. PLoS ONE 2013, 8, e72539.
(33) Caffeine For The Sustainment Of Mental Task Performance: Formulations For Military Operations. Nutrition Today 2002, 37, 26-27.
(34) Tiffin, P.; Ashton, H.; Marsh, R.; Kamali, F.; Ashton, H.; Marsh, R. Pharmacokinetic And Pharmacodynamic Responses To Caffeine In Poor And Normal Sleepers. Psychopharmacology 1995, 121, 494-502.
(35) Baggott, M.; Childs, E.; Hart, A.; de Bruin, E.; Palmer, A.; Wilkinson, J.; de Wit, H. Psychopharmacology Of Theobromine In Healthy Volunteers. Psychopharmacology 2013, 228, 109-118.
(36) Butcher, R. W.; Sutherland, E. W. Adenosine 3', 5'-phosphate in biological materials. I. Purification and properties of cyclic 3', 5'-nucleotide phosphodiesterase and use of this enzyme to characterize adenosine 3', 5'-phosphate in human urine. The Journal of biological chemistry, 1962, 237, 1264.
(37) Lane, J.; Pieper, C.; Phillips-Bute, B.; Bryant, J.; Kuhn, C. Caffeine Affects Cardiovascular And Neuroendocrine Activation At Work And Home. Psychosomatic Medicine 2002, 64, 595-603.
(38) Smits, P.; Temme, L.; Thien, T. The Cardiovascular Interaction Between Caffeine And Nicotine In Humans. Clinical Pharmacology and Therapeutics 1993, 54, 194-204.
(39) Addicott, M.; Yang, L.; Peiffer, A.; Burnett, L.; Burdette, J.; Chen, M.; Hayasaka, S.; Kraft, R.; Maldjian, J.; Laurienti, P. The Effect Of Daily Caffeine Use On Cerebral Blood Flow: How Much Caffeine Can We Tolerate?. Human Brain Mapping 2009, 30, 3102-3114.
(40) Grome, J.Stefanovich, V. Differential Effects Of Methylxanthines On Local Cerebral Blood Flow And Glucose Utilization In The Conscious Rat. Naunyn-Schmiedeberg's Archives of Pharmacology1986, 333, 172-177.
(41) Hayes,; Lucas,; Shi,. Importance Of Post-Exercise Hypotension In Plasma Volume Restoration. Acta Physiologica Scandinavica 2000, 169, 115-124.
(42) Fekete, A.; Sasser, J.; Baylis, C. Chronic Vasodilation Produces Plasma Volume Expansion And Hemodilution In Rats: Consequences Of Decreased Effective Arterial Blood Volume. AJP: Renal Physiology 2010, 300, F113-F118.
(43) Iijima, T.; Takagi, T.; Iwao, Y. An Increased Circulating Blood Volume Does Not Prevent Hypotension After Pheochromocytoma Resection. Canadian Journal of Anesthesia/Journal canadien d'anesthésie 2004, 51, 212-215.
(44) Balaszczuk, A.; Tomat, A.; Bellucci, S.; Fellet, A.; Arranz, C. Nitric Oxide Synthase Blockade And Body Fluid Volumes. Braz J Med Biol Res 2002, 35, 131-134.
(45) Nette, R. Norepinephrine-Induced Vasoconstriction Results In Decreased Blood Volume In Dialysis Patients. Nephrology Dialysis Transplantation 2006, 21, 1305-1311.
(46) Howraa, A.; Patrick A, B.; Le-Xin, W. Diagnosis And Management Of Postural Orthostatic Tachycardia Syndrome: A Brief Review. Journal of Geriatric Cardiology 2012, 9, 61-67.
(47) Callahan, M.; Gengeliczki, Z.; Svadlenak, N.; Valdes, H.; Hobza, P.; de Vries, M. Non-Standard Base Pairing And Stacked Structures In Methyl Xanthine Clusters. Physical Chemistry Chemical Physics 2008, 10, 2819-2826.
No comments:
Post a Comment